Optimism, but Obstacles Abound for the Future of Malaria Control

PLOS Medicine Specialty Consulting Editor Lorenz von Seidlein reports that highlights from the Pan African Malaria Conference and the Malaria Summit portend a bright future for ending malaria, but first we must deal with current obstacles.
On World Malaria Day 2018, there are many things to be hopeful for. The Multilateral Initiative on Malaria hosted the 7th Pan African Malaria conference from April 15th to 20th in Dakar, Senegal where several drug producers presented information on new anti-malarial candidates. Notably, the Novartis Institute discussed the drug candidates, KAF 156 and KAE 609, which could be licensed in the coming years. Coinciding with the conference The Lancet published a promising report on two vector control products, a long-lasting insecticidal net that incorporates a synergist piperonyl butoxide (PBO) and a long-lasting indoor residual spraying formulation of the insecticide pirimiphosmethyl. Meanwhile at the Malaria Summit in London Bill Gates with a number of governments, international organizations, and members of civil society and the private sector pledged investments worth a collective $4 billion in the continued fight against malaria. Gates announced that gene editing holds great promise as the next technologic solution to the malaria problem. And the director of the Global Malaria Program at the WHO announced new strategies in Dakar to control if not eliminate malaria.
The future may look bright but the current situation is complex. The 2017 WHO World Malaria Report (WMR) indicated for the first time after many years of steady decreases, an increase in the global number of malaria cases from 211 million in 2015 to 216 million in 2016. The report is hampered by the fact that the WHO once more changed its reporting methodology for the 2017 report without giving a clear explanation why and how this was done. As a result the number of cases for previous years have been once more revised in the 2017 report (case burden estimates for 2010 have been revised seven times in as many years!). The inconsistency of reporting methodology makes the trends difficult to interpret and adds doubt to the reliability of the findings.
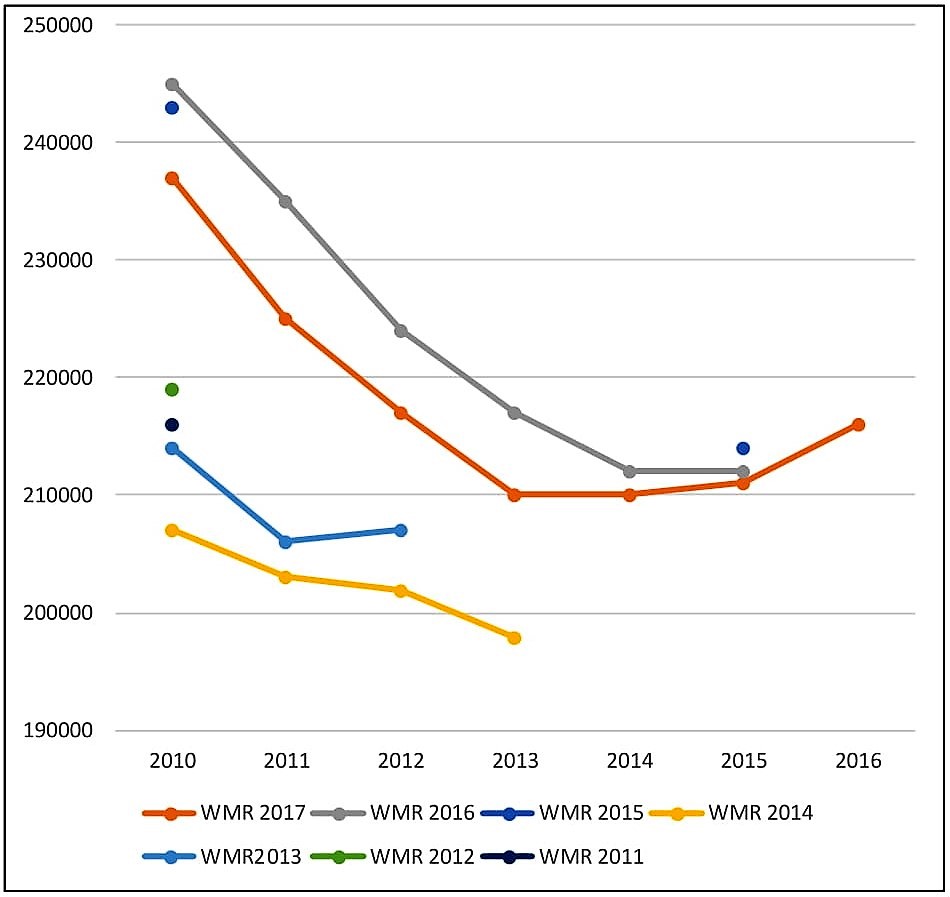
Figure: Estimated malaria cases (in thousands), by year of the World Malaria Report (WMR). Note: in the last 7 WMRs there have been 7 different estimates for the malaria case burden in 2010.
The undeniably heterogeneous malaria burden across countries in sub Saharan Africa further complicates the situation. Twenty years ago The Gambia routinely reported a P. falciparum infection prevalence of around 40% at the peak of the rainy season. Five sub-Saharan countries, including the Gambia, have seen a significant decrease in malaria prevalence, dropping to as low as 0.1% in The Gambia during the 2017 season, whereas 24 high-burden countries saw increases in malaria. Considering the available evidence, it would probably be safer to suggest that trends in malaria burden are mixed.
The technologies presented in Dakar and London hold promise but relying on the potential of new technologies has led to disappointment in the past, as the dashed hope in an ideal malaria vaccine illustrated. The effectiveness of these newer technologies remain unproven; meanwhile insecticide and antimalarial resistance continue to emerge and spread. Artemisinin-resistant P.falciparum strains have spread from Western Cambodia to Laos and Vietnam. But without definite evidence that the recent increase in malaria cases in the Greater Mekong Subregion (GMS) are directly related to multidrug resistance, the WHO will not declare a public health emergency despite calls to do so. An estimated 0.1% of the global malaria deaths occurred in the GMS in 2016 while roughly USD 300 million (11%) of the annual global spending on malaria (USD 2.7 billion) are spent in the GMS. Some of the experts in Dakar opined that the spending on malaria control in the GMS is way out of proportion, despite historical lessons of chloroquine and sulfadoxine / pyrimethamine resistance emerging from the GMS and entering sub-Saharan Africa in the 1970s to 1990s where it was estimated to cause millions of deaths.
Among the few points on which malaria experts working in Africa and Asia can agree is that access to bednets, early diagnosis and appropriate treatment remain the essential basic control measures. Uninterrupted, universal access to such basic control measures will over time suppress the transmission of malaria. Supplying every household in malaria endemic regions with access to basic control measures should be a common cause around which all parties can rally. But providing such access to the 3.4 billion people globally at risk for malaria will cost more than even Bill Gates can afford. Only a concerted effort of heads of states of affected malaria-endemic countries as well as high income countries can address such a challenge.
Meanwhile in the many conflict zones access to basic control measures remains sporadic or permanently absent. In the centre of Africa, Niger, Chad, Central African Republic and eastern Congo even the most basic reporting of the malaria cases and deaths is unreliable or completely absent. This is a situation which was not discussed, has not been addressed, and will become worse as militarization of these conflict zones increases. Policymakers and intervention forces would be well advised to adopt quickly some of the lessons learned in The Gambia in conflict regions currently neglected by the international malaria programmes.
There are a number threats to malaria control not to mention elimination, including drug and insecticide resistance, disruption of sustained funding, and armed conflicts. But there is also reason for optimism as new antimalarial drugs and vector control technologies could become available. There is a hope that policymakers and the international funders appreciate and can replicate the success in malaria control achieved in a few select countries, like The Gambia.
Lorenz von Seidlein has worked for 20 years on malaria and other issues in global health. Lorenz is currently coordinating a malaria elimination project with the Mahidol Oxford Research unit in Bangkok, Thailand. He is a Specialty Consulting Editor for PLOS Medicine.
Feature Image Credit: US Army Africa, Flickr