American Zika in 2016 and 2017: The Strange Case of Mr. Hyde and Dr. Jekyll

As North America heads into summer, Peter Hotez, co-Editor-in-Chief of PLOS Neglected Tropical Diseases, discusses the risk for Zika outbreaks and hopes Mr. Hyde doesn’t rear his ugly head.
In 1886 Mr. Robert Louis Stevenson published a novella, entitled [the] Strange Case of Dr. Jekyll and Mr. Hyde, about the dual personalities of the friendly and amiable Dr. Henry Jekyll and his evil counterpart Edward Hyde. In some ways we’re seeing a similar scenario play out with Zika virus infection.
In early 2016, a wave of Zika virus infection swept through South America, causing almost 400,000 cases, with more than one-half in Brazil, and almost 100,000 cases in Colombia, and 60,000 in Venezuela. A second wave of Zika virus infection rolled into the Caribbean later that year, causing around 40,000 cases each in Puerto Rico and Martinique, and elsewhere. In regards to the United States, we now know from molecular clock data published recently in Nature, that it was during this period that Zika virus entered South Florida through multiple entries from the Caribbean, with transmission propagated by local Aedes aegypti mosquitoes. A second autochthonous focus of Zika virus infection occurred in South Texas and may have entered from Mexico.
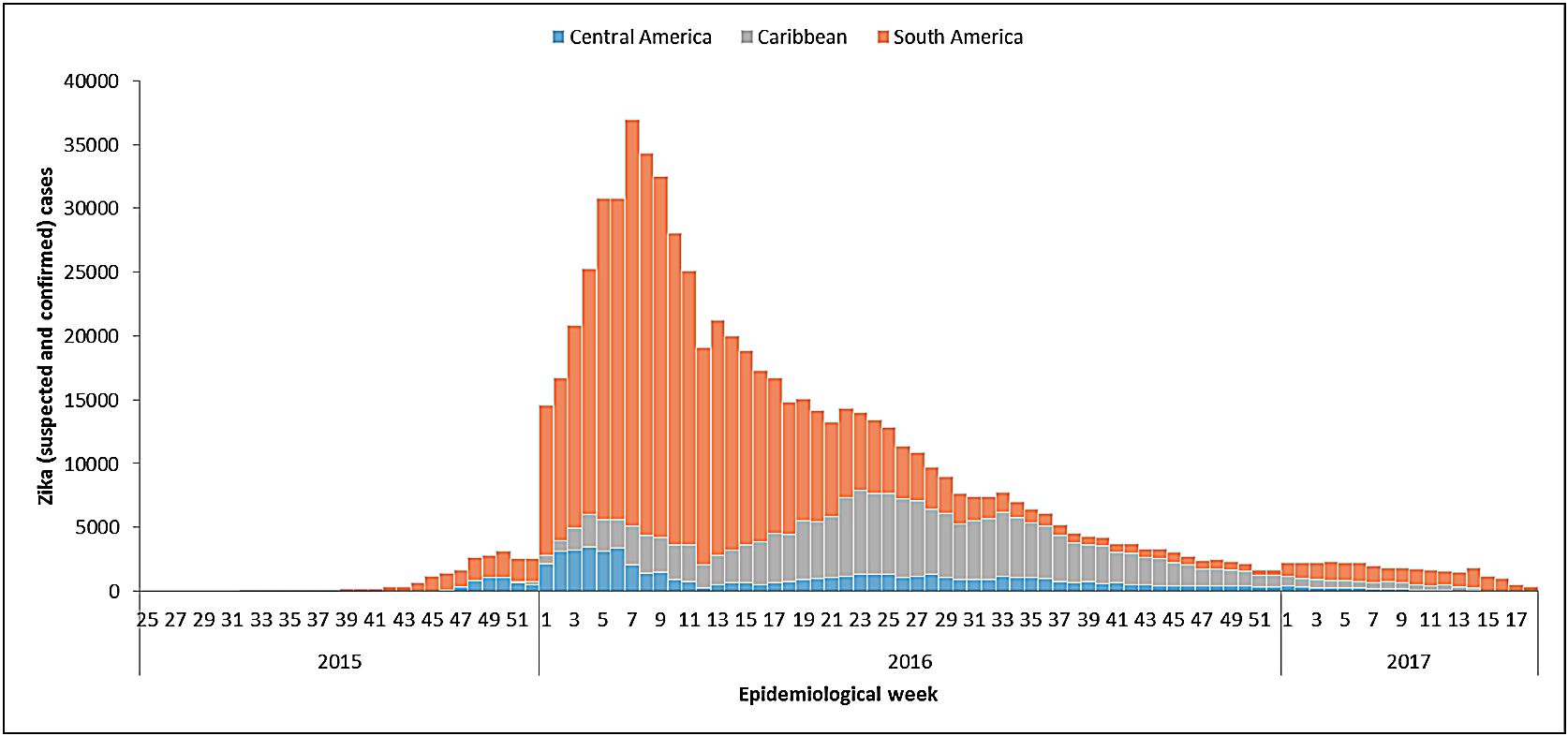
As shown in Fig. 1, which was prepared by PAHO-WHO, the dramatic rise of Zika in 2016 was followed by an equally dramatic decline by the end of 2016. As we moved into 2017 the Zika epidemic in the Latin America and Caribbean region had almost ended. Mr. Hyde had mostly vanished!
{kind=link}
Fig. 1. Distribution of suspected and confirmed Zika cases by epidemiological week and sub-region. Region of the Americas, 2016 – 2017 (as of EW 18)
The basis for this decline will require an extensive investigation, but a likely explanation will include significant herd immunity developing among the newly infected populations in the Americas, which then failed to sustain virus transmission.
Shown in Fig. 2 is additional information from PAHO-WHO for where we stand today in terms of Zika in the Americas. While countries such as Brazil no longer seem to be sustaining new transmission, there are new foci popping up in additional Latin American countries, including Ecuador and Peru on the Pacific Coast of South America, as well as in Argentina and Bolivia.
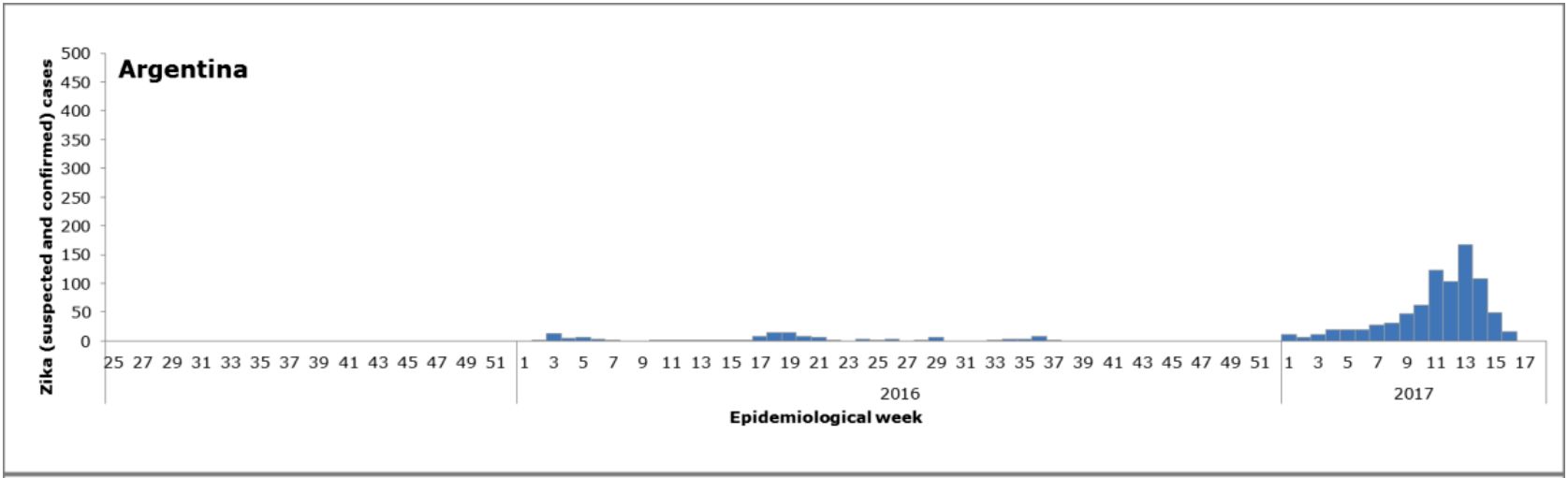
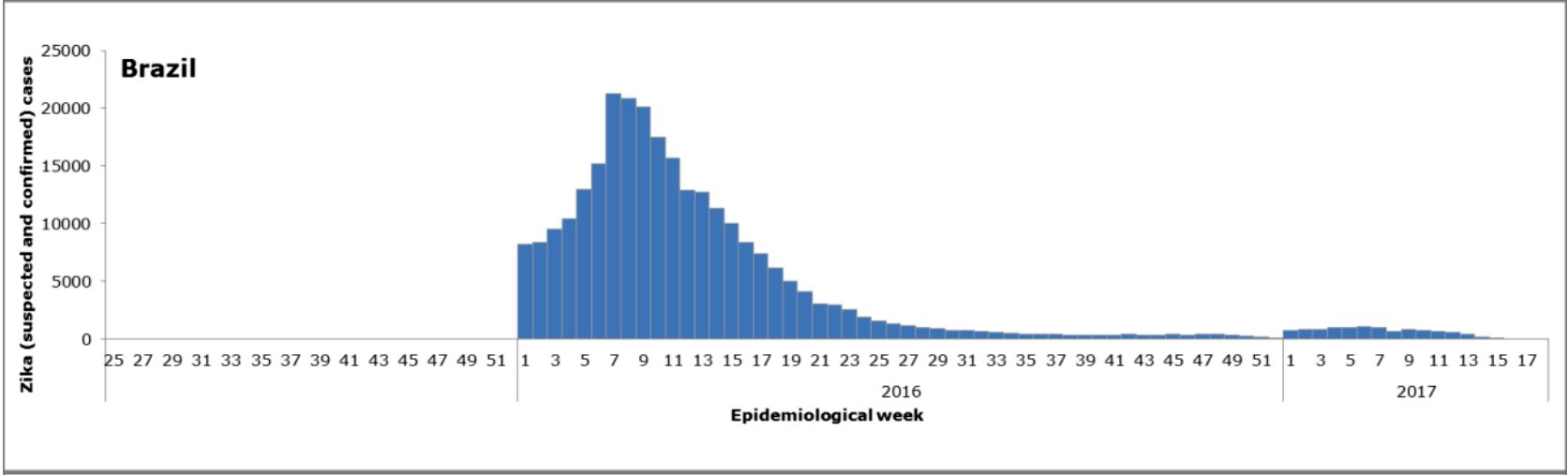
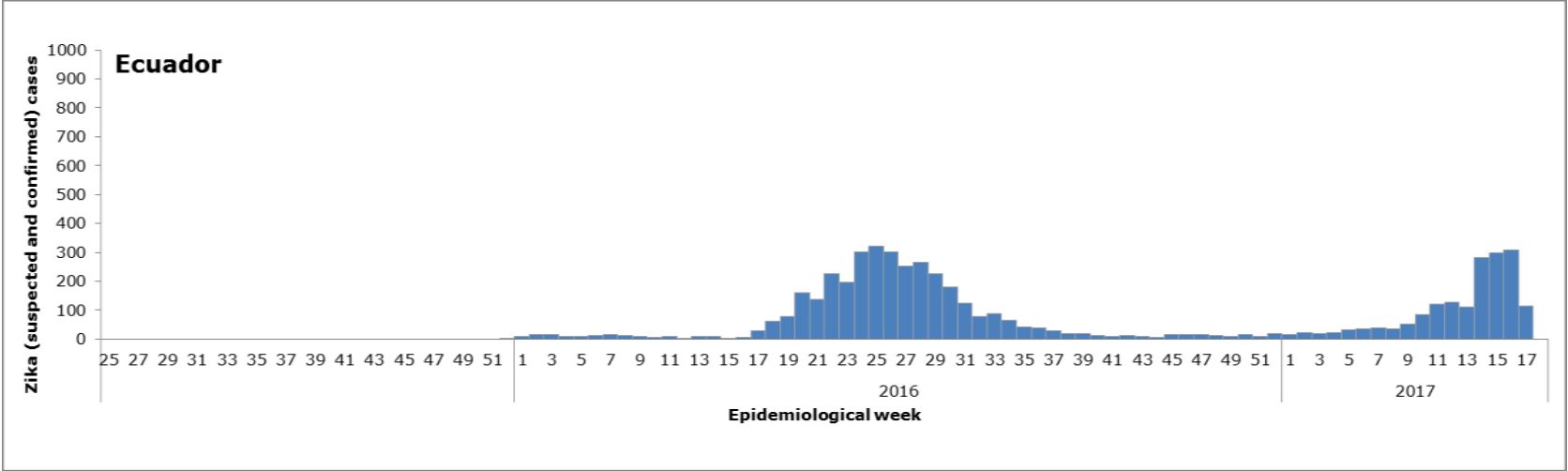
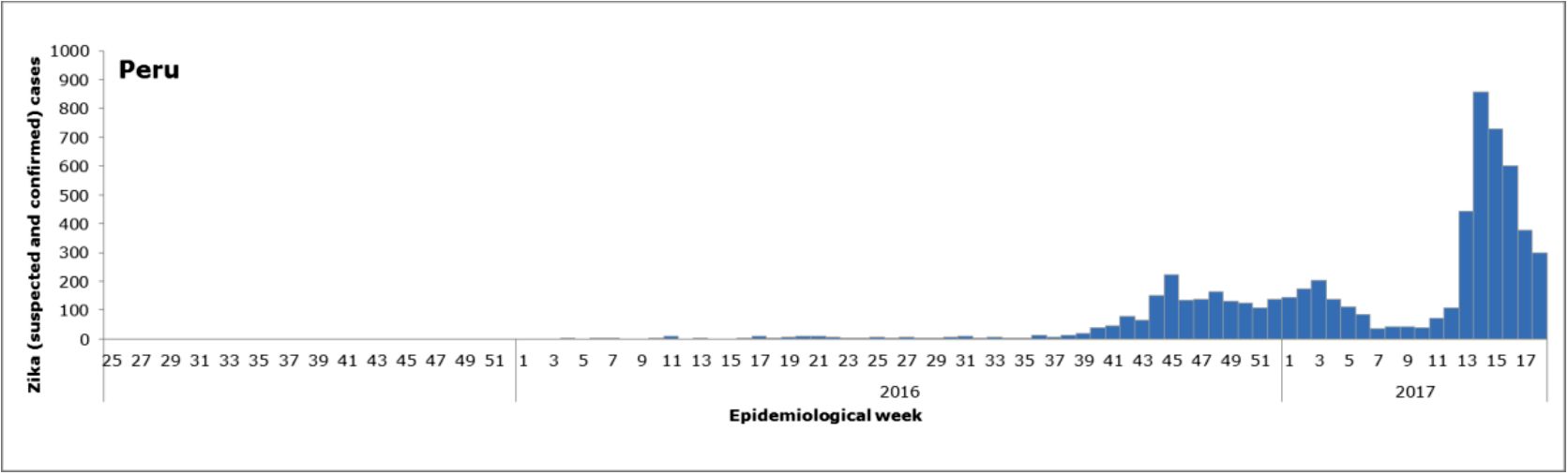
Fig. 2. Distribution of suspected and confirmed Zika cases by EW. Argentina, Brazil, Ecuador, and Peru, EW 25 of 2015 to EW 18 of 2017. Reprinted from Regional Zika Epidemiological Update (Americas) May 25, 2017 with permission from PAHO/WHO, original copyright PAHO/WHO 2017.
What will these disease patterns portend for North America as we move into the summer months? It’s pretty clear that overall transmission is significantly down in the Western Hemisphere. In terms of South Florida since there does not seem to be a high level of Zika virus transmission in the Caribbean (that served as the source of last year’s epidemic), we may indeed not see a return of Zika to Florida. So in Florida anyway, Dr. Jekyll may have finally overpowered Mr. Hyde!
On the other hand, for Mexico, I think it remains to be seen given that their traditional rainy season (and therefore mosquito season) goes from June to October, so we’ll still need to be vigilant for the return of Zika virus infection there. And since Mexico and South Texas are linked in so many ways, we need to continue monitoring Zika virus infection. Still another concern is that this past winter has been record-setting in terms of its mildness and high temperatures, which means that Aedes aegypti numbers could be high in Texas urban areas such as San Antonio and Houston. For all these reasons, what will happen in terms of Zika virus infection in Texas may still be anyone’s guess. Compounding this problem is the fact that four other arboviruses transmitted by Ae aegypti – dengue, chikungunya, Mayaro, and yellow fever – remain circulating in the Americas, so that we need to be on the lookout for their emergence in North America as well.
Finally, other outstanding questions are in regards to new technologies for Zika and other arbovirus infections. Will the overall decline in transmission reduce their urgency and throw cold water on investments for GMO mosquitoes or vaccines? I hope not, because one of the lessons learned about arbovirus infections, such as West Nile virus infection and dengue is that they do eventually return. So even if Zika virus does not return in a big way to the Western Hemisphere in 2017, there’s still 2018, 2019, or 2020, and so forth.
I’ve said previously that we’re in a “new normal” when it comes to arbovirus transmission in the Americas. We now have at least six major arboviruses that could re-emerge at any time, so moving forward I believe there will be a high level of urgency to develop multivalent technologies, including multivalent vaccines that can prevent infection from multiple arboviruses simultaneously.