Chagas Disease: The New Numbers

Peter Hotez (@PeterHotez), Co-Editor in Chief of PLOS NTDs, comments on new WHO estimates of the burden of Chagas disease in Latin America.

The World Health Organization (WHO) has just released new estimates on the number of people living with Chagas disease (American trypanosomiasis caused by Trypanosoma cruzi) in Latin America by country (for the year 2010), together with estimates on new cases due to vectorial, maternal-to-child, and blood transfusion transmission (pdf available here). Shown in Tables 1 and 2 is my summary and ranking of some of these data.
Today the largest numbers of people living with Chagas disease live in Argentina, Brazil, and Mexico, followed by Bolivia and Colombia (Table1). Similarly, Argentina and Brazil lead in the number of cases of Chagasic cardiomyopathy, although more cases are found in Colombia and Bolivia than in Mexico.
Table 1. Ranking of countries by the number of people living with Chagas disease and Chagasic cardiomyopathy.
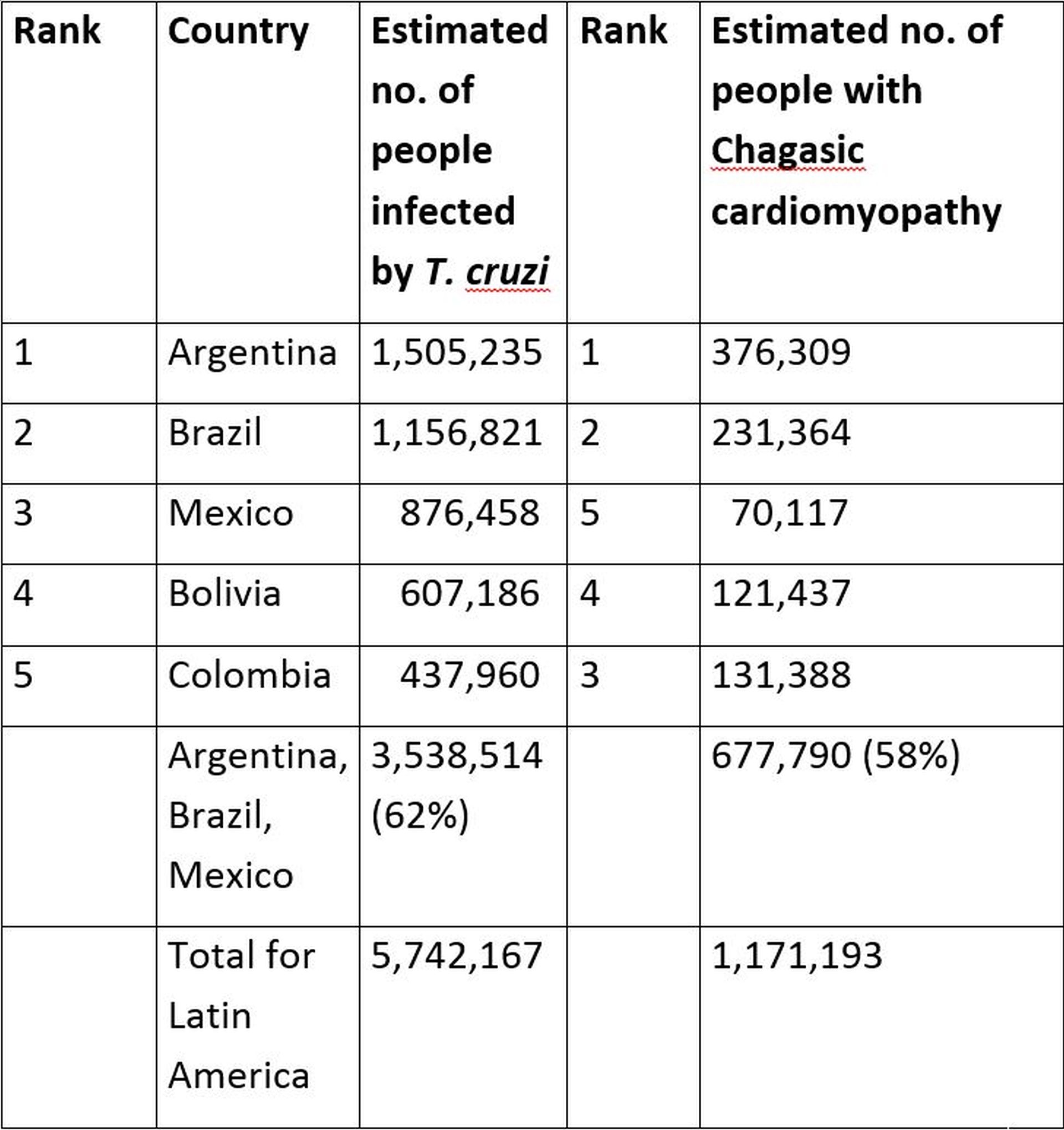
Overall, the three wealthiest economies in Latin America, each group of 20 (G20) countries, account for most (62%) of the people living with Chagas disease in the region, and most (58%) of the cases of Chagasic cardiomyopathy. Moreover, Mexico has the largest numbers of cases of congenital Chagas disease resulting from maternal-to-child transmission, followed by Argentina (data not shown). I have used the term “blue marble health” to describe high concentrations of poverty and neglected tropical diseases in G20 and other wealthy nations. Also relevant to the concept of blue marble health is that fewer than one percent of people living with Chagas disease in Latin American countries, including wealthy economies, receive or have access to treatment for their T. cruzi infections with either benznidazole or nifurtimox.
Shown in Table 2 is a ranking of Chagas disease by prevalence. According to the WHO, overall approximately one percent of the population of Latin America is infected with T. cruzi, but today the highest percentage of T. cruzi infected individuals live in Bolivia, followed by Argentina and Paraguay. The WHO points out that these three countries constitute a part of the Gran Chaco, which must now be considered an important epicenter for Chagas disease in the Americas.
Table 2. Ranking of countries by the prevalence of Chagas disease
| Rank | Country | Estimated prevalence of T. cruzi infection per 100 habitants |
| 1 | Bolivia | 6.104 |
| 2 | Argentina | 3.640 |
| 3 | Paraguay | 2.130 |
| 4 | Ecuador | 1.379 |
| 5 | El Salvador | 1.297 |
| Latin America | 1.055 |
Also, according to the WHO there were approximately 30,000 new cases of Chagas disease as a result of vectorial transmission in 2010, with more than two-thirds of those new cases in just three countries – Bolivia, Mexico, and Colombia [1]. However, high rates of vectorial transmission also occur today in the Andean subregion, especially Colombia, Ecuador, Peru, and Venezuela, and Central America, especially El Salvador, Guatemala, and Honduras [1].
My takeaway messages from these important WHO data include the following:
- Today the largest numbers of people infected with T. cruzi live in Latin America’s wealthiest G20 economies – Argentina, Brazil, and Mexico – and the overwhelming majority of those people do not have access to antiparasitic treatment.
- Bolivia remains “ground zero” for global Chagas disease, in terms of the highest prevalence and vectorial transmission.
- High rates of vectorial and maternal-to-child transmission still occur in the Gran Chaco, the Andean subregion, and Central America.
- Although autochthonous transmission has been documented in the United States by our National School of Tropical Medicine at Baylor College of Medicine and others, cases in the United States were not included in the WHO release, nor were cases resulting from the “globalization” of Chagas disease to Europe, Japan and Australia.
These new WHO data also represent an important wake-up call for global leaders and elected officials. Today, millions of Latin Americans living in poverty are denied access to essential medicines and treatment. They are also mostly denied access to innovation for new drugs and vaccines now in early and mid-stage development by DNDi (and its partners) and our Sabin Vaccine Institute and Texas Children’s Hospital Center for Vaccine Development (in collaboration with the Carlos Slim Foundation), respectively. Finally, while the WHO and its regional office, the Pan American Health Organization, is committed to interrupting the transmission of Chagas in the major affected areas, they need a greater commitment of resources by the G20 economies in the Americas, including financial resources, to aggressively halt the spread of Chagas disease in Bolivia, Gran Chaco, Andean subregion, and Central America.
[…] Peter Hotez (@PeterHotez), Co-Editor in Chief of PLOS NTDs, comments on new WHO estimates of the burden of Chagas disease in Latin America. The World Health Organization (WHO) has just released new estimates on the number of people living with … Continue reading » […]
[…] Read the whole article here […]